Really liked this quick to read CNN article on PPACA impacts in 2013. While most changes will not take affect until 2014, there are a few things to watch out for next year. The big ones include:
1) Increase in Medicaid Provider payments - should be good news for docs
2) Health Insurance Exchanges "Go Live" in Oct. 2013
3) Insurers will have to publish easy to understand brochures describing their plans in a standard format; see sample here.
Sunday, December 30, 2012
Saturday, December 29, 2012
A "Bundled" Surgery: the Perfect Christmas Gift?
Want a free trip to Florida or California from your employer? No problem! Just break a leg (literally).
Kroger and Wal-Mart are among employers now sending their staff on all-expenses paid trips to get medical care. As described in this LA Times article, costs for routine operations can vary widely depending on the care provider. For example, Kroger found that one hospital in particular can provide hip and knee replacement surgeries at up to 15% lower cost than other providers - while maintaining the same quality in care. This savings in cost more than covers the cost of trip expenses to receive care at the hospital, which is located in Irvine, CA. Additionally, there is the element of predictability - employers contract with each selected provider to pay a fixed-rate per surgery, or "episode" of care - the oh-so-trendy "bundled" payment.
Are bundled payments the future of healthcare? I just can't wait to find out - I know you feel the same way!
Kroger and Wal-Mart are among employers now sending their staff on all-expenses paid trips to get medical care. As described in this LA Times article, costs for routine operations can vary widely depending on the care provider. For example, Kroger found that one hospital in particular can provide hip and knee replacement surgeries at up to 15% lower cost than other providers - while maintaining the same quality in care. This savings in cost more than covers the cost of trip expenses to receive care at the hospital, which is located in Irvine, CA. Additionally, there is the element of predictability - employers contract with each selected provider to pay a fixed-rate per surgery, or "episode" of care - the oh-so-trendy "bundled" payment.
Are bundled payments the future of healthcare? I just can't wait to find out - I know you feel the same way!
Monday, September 24, 2012
PPACA excluding Immigrants - Bad Health Policy?
My beloved healthcare bill isn't perfect, as most of the things I love aren't....sigh.
The White House recently disclosed that young immigrants now allowed to stay in the US will not qualify for health insurance under PPACA (neither Commercial nor Medicaid / CHIP public coverage). This is a great example of bad policy stripping away the good intentions of another - these immigrants, now allowed to stay in the US with dreams of becoming productive citizens, will not qualify to purchase health insurance on exchanges and have access to affordable healthcare.
In my public health program, we learned all too often that personal health is very much linked to the ability to become a productive member of society...Ricardo Campos' story in the article is a great examples of this.
You can read the article here.
The White House recently disclosed that young immigrants now allowed to stay in the US will not qualify for health insurance under PPACA (neither Commercial nor Medicaid / CHIP public coverage). This is a great example of bad policy stripping away the good intentions of another - these immigrants, now allowed to stay in the US with dreams of becoming productive citizens, will not qualify to purchase health insurance on exchanges and have access to affordable healthcare.
In my public health program, we learned all too often that personal health is very much linked to the ability to become a productive member of society...Ricardo Campos' story in the article is a great examples of this.
You can read the article here.
Tuesday, August 28, 2012
Shocking!: Medicaid expansions help people, says NEJM
Let's be honest...sometimes it's easier just to jump to the Conclusion:
"Conclusions:
State Medicaid expansions to cover low-income adults were significantly associated
with reduced mortality as well as improved coverage, access to care, and self-reported health."
The New England Journal of Medicine recently published a study comparing 3 states that adopted Medicaid expansions to "control states" that did not. And, apparently after adjusting for all the things you're supposed to adjust for, the expand-States had reduced mortality (esp. among adults ages 35-64), improved access to care, and better self-reported health...
Link: http://www.nejm.org/doi/pdf/10.1056/NEJMsa1202099
"Conclusions:
State Medicaid expansions to cover low-income adults were significantly associated
with reduced mortality as well as improved coverage, access to care, and self-reported health."
The New England Journal of Medicine recently published a study comparing 3 states that adopted Medicaid expansions to "control states" that did not. And, apparently after adjusting for all the things you're supposed to adjust for, the expand-States had reduced mortality (esp. among adults ages 35-64), improved access to care, and better self-reported health...
Link: http://www.nejm.org/doi/pdf/10.1056/NEJMsa1202099
Friday, August 24, 2012
Lessons from the Cheesecake Factory
If you haven't seen it yet, Dr. Atul Gawande has another great New Yorker article on healthcare. This time, he does on deep-dive on the super-efficient restaurant chain, Cheesecake Factory, and basically talks about how healthcare is....well, nothing like that. Click here for the full article (warning; it's long!)
Outside of getting an insider's guide to the wonderful world of Cheesecake Factory operations, I like the story he tells about his mom getting a total knee replacement...you get a sense of the high variation in healthcare, among and even within hospitals....and how some forward-thinking doctors were able reduce variation and give his mother some high-quality healthcare!
Outside of getting an insider's guide to the wonderful world of Cheesecake Factory operations, I like the story he tells about his mom getting a total knee replacement...you get a sense of the high variation in healthcare, among and even within hospitals....and how some forward-thinking doctors were able reduce variation and give his mother some high-quality healthcare!
Monday, August 6, 2012
Healthcare JV's, M&A
Terms like "Joint Venture" and "Mergers and Acquisitions" don't typically come to mind when you think healthcare....well....times are changing:
1) Group Health Cooperative recently formed a Joint Venture with a Catholic Health System in Spokane, WA to provide more efficient healthcare services: http://www.kaiserhealthnews.org/Stories/2012/August/01/group-health-providence-partnership-spokane.aspx
2) Private Equity Firm Ceberus Capital Management now owns Steward Healthcare in Boston, turning it into a for-profit system that is now positioned to compete with big players such as Mass Gen, Brigham....http://www.commonwealthmagazine.org/News-and-Features/Features/2012/Summer/001-Cerberuss-health-care-play.aspx
Is this good for healthcare? I suppose time will tell.
1) Group Health Cooperative recently formed a Joint Venture with a Catholic Health System in Spokane, WA to provide more efficient healthcare services: http://www.kaiserhealthnews.org/Stories/2012/August/01/group-health-providence-partnership-spokane.aspx
2) Private Equity Firm Ceberus Capital Management now owns Steward Healthcare in Boston, turning it into a for-profit system that is now positioned to compete with big players such as Mass Gen, Brigham....http://www.commonwealthmagazine.org/News-and-Features/Features/2012/Summer/001-Cerberuss-health-care-play.aspx
Is this good for healthcare? I suppose time will tell.
Tuesday, July 17, 2012
A "Healthcare Handbook" for Clinicians
New York Times' WellBlog today features 2 Medical students who wrote a book about understanding the US Healthcare system...I am very excited to read this. It helps to define all the fancy new slang, including "Accountable Care Organizations" and "Bundled Payments." May be a good refresher for all those working in healthcare...plus it's only 175 pages long!
http://well.blogs.nytimes.com/2012/07/12/two-medical-students-navigate-the-health-care-maze/?ref=health

http://well.blogs.nytimes.com/2012/07/12/two-medical-students-navigate-the-health-care-maze/?ref=health

Thursday, July 5, 2012
I've Reached a New Height; PDJ and I Aligned
My old Health law professor wrote a spectacular summary of the SCOTUS decision and opinion for Medicare Newsgroup that is eerily similar to my previous post...
Okay, okay...he may have been a little more eloquent in his blog post, and it's much more educational than my piece....but that's why he's Peter D. Jacobson, and I'm not.
Okay, okay...he may have been a little more eloquent in his blog post, and it's much more educational than my piece....but that's why he's Peter D. Jacobson, and I'm not.
Friday, June 29, 2012
Health Reform Lives!

3 quick comments regarding yesterday's events:
1) While good for the Obama campaign, the mandate will inevitably be spun as a new tax on Americans by Romney & Co. (to the effect of $500bn (link) in new taxes according to his televised reaction yesterday)...I wonder where this figure comes from?
2) The NYTimes published an article today about mounting pressures to meet PPACA deadlines (link) Some States, such as WI, are even holding out until November...this just does not seem very smart to me...arrogance > reason:
"Mr. Walker quickly raised the risk by announcing that, in spite of the ruling, he would continue to delay any imposition of the law while waiting to see whether Republicans took control of the White House or Congress in November. Republicans on Capitol Hill, and the party’s presumptive presidential nominee, Mitt Romney, have vowed to repeal the entire law if they gain power."
2) What about Medicaid expansions being left up to the States? There wasn't too much talk about this yesterday, but I think it's an important point...will Health Reform help the poor attain health insurance? From ABC:
"Renee M. Landers of Suffolk University Law school says the impact of today’s ruling, “could reduce the number of people who will be eligible for Medicaid because it is easier for the states to opt out.”"
I suppose we'll find out in time. Regardless, Team Obama has made history...and some pretty Healthy Health Policy!
Friday, June 8, 2012
The Behavioral Health Medical Home (this is exciting)
The
Patient-Centered Medical Home (PCMH) is like my younger brother, Kevin – it get
tons of attention despite having very little proof of adding any value to
society (okay, a bit of exaggeration – the PCMH (not my brother) has shown some
promising results over time). However,
the idea of a specialty care medical home
is talked about much less, but could serve a very important role in
managing the needs of specific patient populations.
How about going even further, and introducing the
concept of a Behavioral Health Medical
Home (BHMH)? Does this mean that a
patient who experiences chronic mental illness that lacks primary care services
or vice versa could get whatever he or she needs all in one place, you
ask? Why yes…I believe it does! And it’s already being done at Cherokee
Health System (CHS) in Tennessee. (
I’m completely
impressed by CHS's integrated behavioral health program – what a practical solution to managing a complex
patient population. CHS recognized early
on that the needs of those with Severe Mental Illness (SMI) are very unique,
and exacerbated by the fact that (especially for Medicaid patients) there is
lack of social supports necessary to managing their conditions. The case for a behavioral health medical home
that integrates primary care is strong:
- Research has shown more mental health interventions occur
in primary care than in specialty mental health settings
- Over one-third of patients in most primary practices have
a psychiatric disorder
- PCP's often feel inadequate in addressing the behavioral health needs of their patients
- Treating mental health in the primary care setting may allow patients to overcome the stigma associated with receiving behavioral healthcare
- 80% of people with mental illnesses have 3+ chronic
conditions
- Those with SMI have high rates of diabetes, hypertension, obesity, and hyperlipidemia (this is often a side-effect of newer antipsychotic drugs)
Typical Service Scenario: The
PCP determines that psychosocial factors underlie the patient’s presenting
complaints or are adversely impacting response to treatment. During the visit, the PCP “hands off” the
patient to the BHC for consultation services (e.g., suicide risk assessment,
anxiety and anger management, substance abuse intervention)
Insurers such as BCBS of Tennessee are already taking notice of some very
positive results, that include reduced ER utilization, lower costs per patient,
and fewer hospital admissions. In
addition, CHS has identified an unconventional revenue stream by offering BHMH
integrated care training to other providers.
In short, the industry has taken note of the BHMH’s success.
“TN has a provider champion – Cherokee Health Systems – that is a
nationally recognized model for primary and behavioral health integration” – National Academy for State Health Policy
State Medicaid programs take note: The National Alliance on Mental
Illness has stated that Medicaid comprises over 50% of overall public mental
health spending (link). With States making moves to tighten budgets,
they should focus on programs that can do more with less – why not start with a
BHMH?
Saturday, May 5, 2012
No Comparing on Hospital Compare
Among the
many interesting things that comprise the extremely exciting life I lead are hours
of browsing the Hospital Compare website
which provides publicly reported quality metrics for U.S. hospitals. The site displays several measures, including
process of care, outcomes, and patient satisfaction scores among the Medicare
population. The user can also select up
to 3 hospitals to do a side-by-side comparison of all the metrics. While using the site, I found it informative,
fairly easy to use/understand, and a powerful tool for all participants in
healthcare – hospitals, clinicians, health insurers, and of course, patients.

Here’s the
thing: I might just be the only who does.
A March 2012 Health Affairs study found that “Medicare’s
seven-year public reporting initiative for hospitals, Hospital Compare, had no
impact on reducing death rates for two key health conditions and just a modest
effect on a third. [This] raises questions about the initiative’s ability to
improve the quality of care provided by the nation’s hospitals.”
Whaaat? All this effort, all this reporting, and no
one’s using the data. I think I’m having
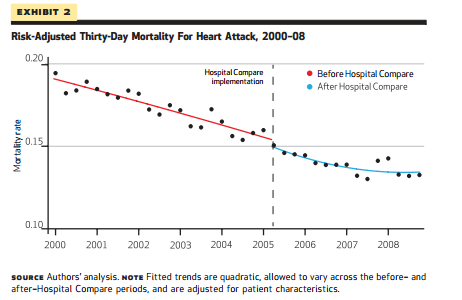
a heart attack (and there’s no time to check the website!) The study also notes that when Hospital
Compare was rolled out in 2005, “there was no comparable control group of
hospitals that were not exposed to the program.
Thus, even if mortality has declined since the introduction of this program,
it could be that these improvements were the result of other innovations in
clinical care that fueled secular trends toward better outcomes in general, and
not the program itself.” Indeed,
clinical outcomes for risk-adjusted mortality rates declined during the time
period for which the study was conducted, but only continued to follow
pre-existing trends:
In
addition, “past surveys have suggested that quality report cards like Hospital
Compare are underused by patients and ignored by referring physicians. This
study adds to that evidence suggesting that consumers at least did not seem to
be checking the Medicare website to make more informed choices about where to
check in for an elective procedure.”
It is unclear to me whether this is simply a lack of awareness, or
checking a website with published readmission rates and measures indicating
whether a beta blocker was appropriately provided really helps the consumer at
all. I recently used Yelp to find my
PCP, and found it to be incredibly helpful to hear user reviews. Maybe, at the end of the day, people want to
hear what their friends and family, not what CMS, has to say about hospitals.
Regardless
of the study’s findings, the website exists, and hospital quality departments
are not going away any time soon.
Indeed, they have played a key role in helping to attain Joint
Commission accreditation, implementing quality initiatives, and of course,
publicly reporting quality data. But
could they be doing more? Given the challenging
environment hospitals are faced with and will continue to face in the next 5-10
years, why not use something that is already required to your advantage, as much as possible? For instance, they could…
1)
Brag about it: If you’re outperforming other hospitals in your region on certain
metrics, especially those related to patient satisfaction, market that! People like things that other people
like. Show this off.
2)
Bring it to payer negotiations: Tell health insurers why you should be the provider of choice, what
you’ve done to improve quality of care, and why patients want you in their
networks.
3)
Use it to attract the best workforce: The Health Affairs study found that quality metrics had no effect on
referrals. But maybe physicians should
start caring – and the hospital can play a role in this. Why wouldn’t a physician want to come and
practice medicine at a place that has solid processes in place to achieve best-in-class
patient safety metrics? Or where
patients are happy with the facilities and nursing staff? And clinicians are not limited to physicians. Nurses, physician extenders and
administrative staff might be attracted to a place that scores well on process
and outcomes metrics.
Would
love to hear your thoughts. Is it not a
shame that there is so much data not
being used to its full potential?
Sunday, February 26, 2012
Can't we call it "Rombama Care" and all just get along?
“There was a study that just came out about 10 days ago, two weeks ago, that listed 15 ways in which Romneycare was the model for Obamacare.” -Rick Santorum; Presidential hopeful, GOP candidate, word mumbler.
In response, Mitt Romney reiterated his intent on repealing Federal Health Reform if he were to win the Presidential nomination. (If interested, you can see the transcript of the debate, here).
This begs the question: Has Massachusetts Health Reform been successful? According to a study published in Health Affairs last month, the answer appears to be yes. Of course, this all depends on how one defines success, but there are some impressive results for fairly standard metrics when evaluating whether or not a health policy is working well for the issues it intended to address.
The study used data from the Massachusetts Health Reform Survey, which targets adults ages 19-64. Health Affairs used data collected between 2006-2010, and compared health outcomes of post-health reform implementation (2007-2010) to outcomes of adults in 2006.
What the study found was insurance coverage in the state had reached 94.2%, (vs. 77.7% U.S. average), decrease in Emergency Department visits and Inpatient stays, and higher self-reported health status. In addition, the fear that public coverage would lead to the end of employer-sponsored insurance (e.g. “crowd out,”) didn’t happen – “Massachusetts’ high level of insurance coverage reflects high levels of employer-sponsored coverage in the state, which remained strong in 2010. More than two-thirds of nonelderly adults (68.0 percent) reported coverage through an employer. This is significantly higher than the level in 2006 (64.4 percent), before health reform.”
Increases in Primary Care utilization were also up 5.9 percentage points, an important shift for population health improvement.
Also, if you want a preview of what Health Reform’s Exchanges may look like, check out Massachusetts’ HealthConnector, the State’s website for those “shopping” for health insurance. I logged in the other day to test its ease of use (it’s easy!) and found that as an individual in her 20’s I could get a plan with a monthly premium of anywhere between $250 to $460, depending on the level of coverage I want.
You can check it out here; https://www.mahealthconnector.org/portal/site/connector/
Of course, similar to Federal Health Reform, MA Health Reform does little to address rising health care costs. “Massachusetts continues to struggle with escalating health care costs, reflecting the decision to defer addressing costs in the 2006 legislation so as not to hold up the expansion in coverage."
Generally speaking, I find these results promising and an important benchmark for what can happen as a result of Federal Health Reform. Some concluding thoughts:
1) Expanding health insurance coverage increased use of preventive care, decreased ED and IP visits, and led to better self-reported health outcomes. This seems like a no brainer to me – if given coverage, people will not wait until they are so sick that they have to go directly to the ED, and keeps them out of the hospital.
2) While MA health reform did not specifically address ways to reduce healthcare costs (e.g. a shift away from fee-for-service), it likely helped set in motion efforts by both payors and providers in the State to think of more efficient ways of delivering care (check out BCBS MA’s AQC initiative, as an example.)
3) What works in MA will work differently in other States. “Of course, the trajectory of policy and health reform will vary across the states, given the wide differences in their political, economic, and cultural environments and the wide range in the different states’ starting points.”
So, for the sake of healthcare, for the sake of the health of the American People, can we just call it "Rombama Care," (catchy, isn't it?) take health reform off the table in the Presidential debates, and all just get along? (and maybe focus on how the heck we can get things like bundled payments to work)?
Tuesday, January 3, 2012
Hospital Hotels
According to this article in today’s New York Times, several illegal immigrants and homeless in New York City are staying in the city’s hospitals for extended stays due to a state law that prohibits public hospitals from discharging patients to shelters or the street. “Patients fit to be discharged from hospitals but having no place to go typically remain more than five years,” said LaRay Brown, the senior vice president for the city’s Health and Hospitals Corporation.
While several public hospitals have a mission to serve their communities and provide care for those in need, allowing patients to stay for such an extended period of time is extremely costly to our healthcare system. “Care for a patient languishing in a hospital can cost more than $100,000 a year, while care in a nursing home can cost $20,000 or less.” But nursing homes are reluctant to accept such patients, and aren’t required by any laws to do so.
Did this slip through the policy cracks? Is this the Charlie Wilson’s War of healthcare? It appears the New York state law was created in isolation, without fully taking into consideration the consequences of its provision. What can be done? Eliminating the law would save the system millions of needed dollars in a time when public institutions already have unsustainable operating margins, but what would be the point of providing someone care then leaving them with nowhere to go and possibly suffer even worse health conditions? Perhaps policymakers can re-visit the standards they set for nursing homes and home health care institutions. But even more importantly – why don’t we just get these people insured?
Subscribe to:
Comments (Atom)